
Your body sends signals long before a disease becomes critical. Foamy urine in the morning. Persistent fatigue that no amount of sleep fixes. Ankles swelling by evening. Most people dismiss these as routine discomforts — stress, poor diet, or ageing. But when these signs appear together, your kidneys may be trying to tell you something serious.
Chronic Kidney Disease, commonly known as CKD, is a condition where the kidneys gradually lose their ability to filter waste and excess fluid from the blood. It is silent, slow-moving, and alarmingly common. In India alone, an estimated 17% of the urban population shows some form of kidney dysfunction — and a large proportion of them remain undiagnosed until the disease reaches an advanced stage.
The good news? CKD is manageable — especially when caught early. And early detection begins with knowing what to look for and, more importantly, what diagnostic tests to ask for.
What Exactly Is Chronic Kidney Disease?
The kidneys are two fist-sized organs located in the back of your abdomen. Every day, they filter approximately 200 litres of blood, removing waste products and excess water as urine. They also regulate blood pressure, balance electrolytes, and produce hormones that stimulate red blood cell production.
Chronic Kidney Disease is a long-term condition characterised by the progressive loss of this filtering capacity. Unlike acute kidney injury (which can occur suddenly due to illness or injury and may be reversible), CKD develops slowly — often over years — and the damage is largely irreversible.
CKD is defined by the presence of kidney damage or a reduced kidney filtration rate (measured as GFR — Glomerular Filtration Rate) that persists for more than three months.
What Causes CKD?
Understanding the root cause of CKD is important because it directly influences the treatment approach and how aggressively the disease needs to be managed.
The most common causes include:
Diabetes mellitus (Diabetic Nephropathy): High blood sugar damages the tiny blood vessels inside the kidneys over time. Diabetes is the single leading cause of CKD worldwide.
Hypertension (High Blood Pressure): Uncontrolled blood pressure exerts excessive force on kidney blood vessels, causing progressive damage.
Glomerulonephritis: Inflammation of the kidney's filtering units (glomeruli), often triggered by immune conditions.
Polycystic Kidney Disease (PKD): A genetic disorder where fluid-filled cysts develop in the kidneys, replacing healthy tissue.
Recurrent Kidney Infections (Pyelonephritis): Repeated infections that scar the kidney tissue over time.
Obstructive Uropathy: Blockages in the urinary tract (from stones, enlarged prostate, or tumours) that cause back-pressure damage.
Lupus and Autoimmune Diseases: Conditions like systemic lupus erythematosus (SLE) can directly attack kidney tissue.
Long-Term NSAID Use: Overuse of painkillers such as ibuprofen or diclofenac can be nephrotoxic over extended periods.
Recognising the Symptoms of CKD
One of the most challenging aspects of chronic kidney disease is that it often produces no noticeable symptoms in its early stages. The kidneys have significant reserve capacity — they can continue functioning adequately even when a substantial portion of their tissue has been damaged.
Symptoms typically become more prominent as the disease progresses. Here is what to watch for:
Early-Stage Symptoms (Often Subtle or Absent)
Slightly foamy or bubbly urine (a sign of protein leakage)
Mild swelling in the feet or ankles
Fatigue or low energy without a clear cause
Increased frequency of urination, especially at night (nocturia)
Occasional changes in urine colour (darker or paler than usual)
Mid-to-Late Stage Symptoms
Persistent nausea or loss of appetite
Unexplained weight loss
Difficulty concentrating or mental fog
Itching (pruritus), particularly at night
Muscle cramps, especially in the legs
Shortness of breath (due to fluid accumulation in the lungs)
Significant swelling in the legs, feet, and around the eyes
High blood pressure that becomes difficult to control
Decreased urine output (in advanced stages)
Important Note: Many of these symptoms overlap with other conditions. A clinical diagnosis based on laboratory tests — not symptoms alone — is essential to confirm CKD.
The Stages of CKD: Understanding Disease Progression
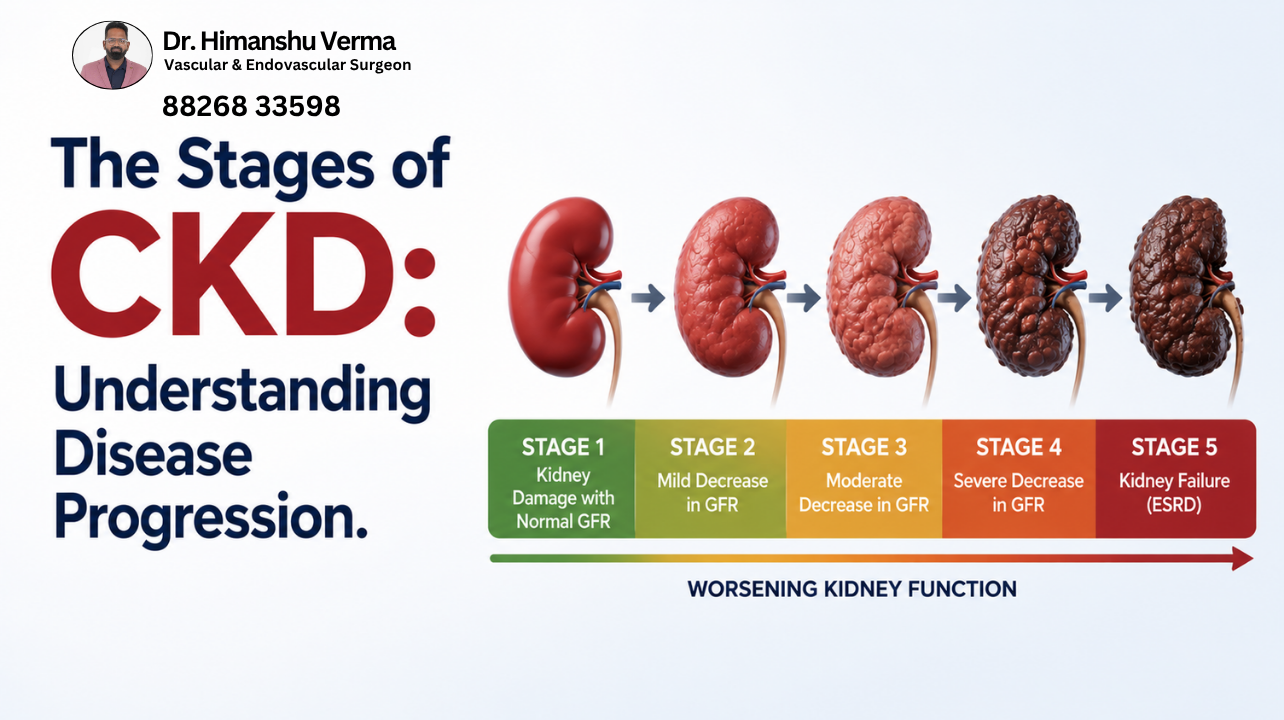
CKD is classified into five stages based on the Glomerular Filtration Rate (GFR), which measures how efficiently your kidneys are filtering blood. Understanding the stage of your CKD helps determine the appropriate treatment strategy and how closely your kidney function needs to be monitored.
Stage | GFR (mL/min/1.73m²) | Description |
Stage 1 | ≥ 90 | Normal or high GFR with evidence of kidney damage (e.g., protein in urine) |
Stage 2 | 60–89 | Mildly decreased GFR with markers of kidney damage |
Stage 3a | 45–59 | Mildly to moderately decreased kidney function |
Stage 3b | 30–44 | Moderately to severely decreased kidney function |
Stage 4 | 15–29 | Severely decreased kidney function |
Stage 5 | < 15 | Kidney failure (End-Stage Renal Disease / ESRD) — dialysis or transplant required |
In Stages 1 and 2, most patients have no symptoms at all. This is precisely why routine screening for at-risk individuals — those with diabetes, hypertension, or a family history of kidney disease — is so critical.
Diagnosis of CKD: The Core of This Discussion
Early and accurate diagnosis of CKD is the single most important step toward slowing its progression and preventing complications. Diagnosis is not based on any one test — it requires a combination of urine tests, blood tests, imaging studies, and clinical assessment over a defined period of time.
Let us walk through each diagnostic category in detail.
1. Urine Tests
Urine analysis is often the first and most accessible clue that something is wrong with the kidneys.
a) Urinalysis (Routine Urine Examination)
This is the most basic screening test. A urine sample is examined for the presence of:
Protein (Proteinuria): Healthy kidneys retain proteins in the blood. When the glomerular filtration barrier is damaged, proteins — especially albumin — leak into the urine. Proteinuria is one of the earliest and most significant markers of CKD. Even trace amounts of protein in urine should not be dismissed.
Blood (Haematuria): Red blood cells in the urine may indicate glomerular disease, kidney stones, or infection.
Glucose: Glucose in the urine despite normal blood sugar can suggest tubular dysfunction.
Casts: Microscopic cylindrical particles formed from proteins or cells. Their type (granular, waxy, red cell casts) provides clues about the nature and severity of kidney disease.
White Blood Cells: A sign of infection or inflammation within the urinary tract.
b) Urine Albumin-to-Creatinine Ratio (UACR) — The Gold Standard for Proteinuria Detection
A random (spot) urine sample is used to measure the ratio of albumin to creatinine. This test corrects for urine concentration and is the preferred method for detecting and quantifying proteinuria in CKD screening.
UACR Value | Interpretation |
< 30 mg/g | Normal |
30–300 mg/g | Moderately increased (microalbuminuria) — early CKD marker |
> 300 mg/g | Severely increased (macroalbuminuria) — significant kidney damage |
Persistent UACR above 30 mg/g on two or more occasions, at least three months apart, confirms clinically significant proteinuria and is a key diagnostic criterion for CKD.
c) 24-Hour Urine Protein Collection
In some clinical situations — particularly when the degree of protein loss needs precise quantification — a 24-hour urine collection is recommended. All urine produced over a full 24-hour period is collected and tested. A result above 150 mg/day of protein is considered abnormal; values above 3.5 g/day indicate nephrotic-range proteinuria, suggesting more severe glomerular disease.
d) Urine Protein Electrophoresis (UPEP)
When the type of protein being lost needs to be identified — especially to rule out conditions like multiple myeloma — UPEP is used. This test separates proteins in the urine based on their molecular weight and electrical charge.
2. Blood Tests

Blood tests for chronic kidney disease including CBC, serum creatinine, electrolytes, and eGFR.
Blood tests provide quantitative data on how well the kidneys are functioning as filters.
a) Serum Creatinine
Creatinine is a waste product generated by normal muscle metabolism. Healthy kidneys filter creatinine efficiently from the blood. When kidney function declines, creatinine accumulates in the bloodstream.
Normal ranges:
Men: 0.7–1.3 mg/dL
Women: 0.5–1.1 mg/dL
However, serum creatinine is not a perfect standalone marker. Its levels are influenced by muscle mass, age, sex, and diet. A muscular young man and an elderly woman may have very different creatinine levels despite having identical kidney function.
This is why creatinine is used in a formula — not read in isolation.
b) Estimated Glomerular Filtration Rate (eGFR) — The Most Important CKD Diagnostic Number
The eGFR is calculated from the serum creatinine level using standardised equations (such as the CKD-EPI or MDRD formula) that factor in age, sex, and sometimes race. It estimates how many millilitres of blood the kidneys can filter per minute per 1.73 m² of body surface area.
eGFR is the primary number used to stage CKD (as shown in the table earlier).
eGFR ≥ 60 with normal urinalysis → likely normal kidney function
eGFR 45–59 → Stage 3a CKD, requires monitoring and lifestyle intervention
eGFR 15–29 → Stage 4 CKD, nephrologist referral and preparation for renal replacement therapy
eGFR < 15 → Stage 5 / End-Stage Kidney Failure
An eGFR below 60, persisting for more than three months, is diagnostic of CKD regardless of whether structural kidney damage is visible.
c) Blood Urea Nitrogen (BUN)
Urea is another nitrogenous waste product. Elevated BUN alongside elevated creatinine suggests reduced kidney filtration. However, BUN can also be raised by high protein intake, dehydration, or gastrointestinal bleeding — so it must be interpreted in context.
The BUN-to-Creatinine ratio (normal: 10–20:1) helps differentiate pre-renal causes (dehydration, reduced blood flow) from intrinsic kidney disease.
d) Complete Blood Count (CBC)
CKD has broad systemic effects. A CBC is essential to identify:
Anaemia: The kidneys produce erythropoietin, a hormone that stimulates red blood cell production. In CKD, this is impaired, leading to anaemia of chronic disease. A low haemoglobin level in a CKD patient is a clinical red flag.
Elevated white cell count: May suggest infection or an inflammatory cause of CKD.
Platelet abnormalities: Uraemia (high urea levels) can impair platelet function.
e) Serum Electrolytes
As kidney function declines, the ability to regulate electrolytes becomes impaired:
Potassium (K⁺): Hyperkalaemia (elevated potassium) is common in CKD and can be life-threatening due to its effects on cardiac rhythm.
Sodium (Na⁺): Hyponatraemia can occur due to fluid retention.
Bicarbonate (HCO₃⁻): Reduced bicarbonate indicates metabolic acidosis — a common complication of CKD as the kidneys lose the ability to excrete acids.
Phosphate and Calcium: Disturbed calcium-phosphate balance leads to renal osteodystrophy (bone disease) and cardiovascular complications in advanced CKD.
f) Serum Uric Acid
Elevated uric acid is both a consequence and a potential contributing factor in CKD progression. It is routinely checked during CKD evaluation.
g) Fasting Blood Sugar and HbA1c
Given that diabetes is the leading cause of CKD, blood glucose and HbA1c (which reflects average blood sugar over three months) are essential both in diagnosing the underlying cause and in assessing glycaemic control in known diabetics.
h) Lipid Profile
Dyslipidaemia is common in CKD and significantly elevates cardiovascular risk. A fasting lipid panel (total cholesterol, LDL, HDL, triglycerides) is part of the standard CKD workup.
3. Imaging Studies
Imaging does not measure kidney function but provides critical structural information.
a) Ultrasound of the Kidneys and Urinary Tract (KUB Ultrasound)
This is the first-line imaging investigation in CKD evaluation. It is non-invasive, widely available, and radiation-free.
What it reveals:
Kidney size: Chronically diseased kidneys often become smaller and echogenic (brighter on ultrasound). Reduced kidney size below 9 cm in adults is generally consistent with CKD.
Cortical thinning: The outer layer of the kidney (cortex) becomes thin as functional tissue is replaced by scar tissue.
Cysts: Multiple bilateral cysts suggest polycystic kidney disease.
Obstruction: Hydronephrosis (swelling of the kidney due to blocked urine outflow) indicates obstructive uropathy.
Stones: Calculi in the kidneys or ureters that may be contributing to obstruction or recurrent infections.
b) Doppler Ultrasound of Renal Vessels
This is particularly relevant in a vascular surgery context. Doppler ultrasound evaluates blood flow through the renal arteries and veins. It is the investigation of choice for:
Renal Artery Stenosis (RAS): Narrowing of one or both renal arteries — often due to atherosclerosis or fibromuscular dysplasia — can cause renovascular hypertension and ischaemic nephropathy, a significant and treatable cause of CKD.
Identifying turbulent flow, velocity changes, and resistive indices that indicate vascular compromise.
In patients with refractory hypertension, asymmetric kidney sizes, or CKD of unclear cause, vascular assessment of the renal circulation is a critical diagnostic step — one that lies squarely within the domain of vascular expertise.
c) CT Scan (Non-Contrast)
A non-contrast CT of the abdomen is superior to ultrasound for detecting kidney stones, especially smaller ones. It also provides better anatomical detail of the kidneys, ureters, and surrounding structures.
Contrast-enhanced CT is generally avoided in CKD patients because iodinated contrast agents are nephrotoxic and can cause contrast-induced nephropathy (CIN), further worsening kidney function.
d) MRI of the Kidneys
MRI offers excellent soft-tissue resolution without radiation. It is useful for:
Characterising kidney masses (solid tumours vs complex cysts)
Evaluating renal vein thrombosis
Assessing for renal artery stenosis (MR angiography)
Gadolinium-based contrast agents used in MRI carry a risk of Nephrogenic Systemic Fibrosis (NSF) in patients with advanced CKD (eGFR < 30), so they must be used cautiously.
e) Nuclear Medicine Scans (DTPA / DMSA Scan)
These radionuclide studies provide functional imaging of individual kidneys:
DTPA scan: Measures differential kidney function and urinary drainage — useful in obstruction assessment.
DMSA scan: Detects cortical scarring from pyelonephritis and assesses split renal function.
4. Kidney Biopsy
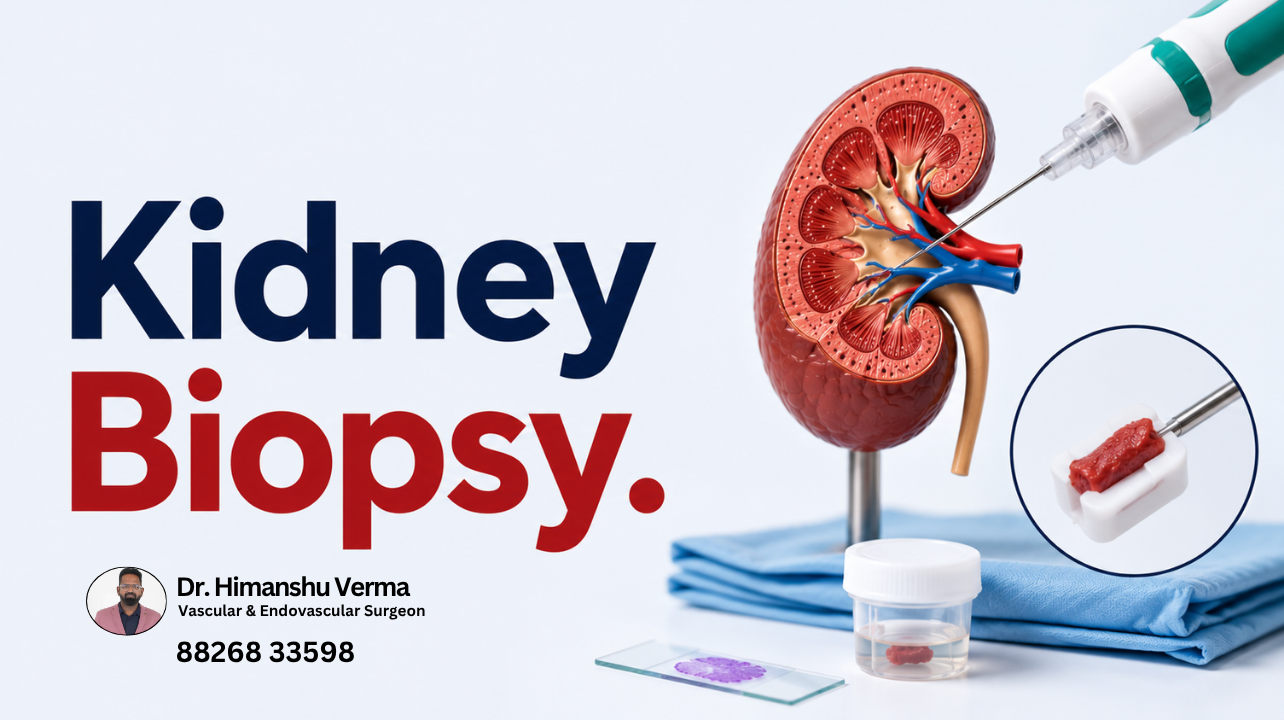
When the cause of CKD cannot be established through non-invasive means, a percutaneous kidney biopsy may be recommended by a nephrologist. A thin needle is guided (usually under ultrasound control) into the kidney to extract a small tissue sample, which is then examined under a microscope.
A kidney biopsy can diagnose:
Glomerulonephritis (various subtypes: IgA nephropathy, membranous nephropathy, focal segmental glomerulosclerosis)
Diabetic nephropathy (when clinical presentation is atypical)
Lupus nephritis
Amyloidosis
Vasculitis affecting the kidneys
A biopsy is not appropriate for all patients. It is generally not recommended in patients with small, shrunken kidneys (as there is little viable tissue to sample and higher bleeding risk) or in those with uncontrolled bleeding tendencies.
5. Additional Specialised Tests
Depending on the suspected underlying cause, further tests may be ordered:
Antinuclear Antibodies (ANA) and Anti-dsDNA: For lupus-related kidney disease
ANCA (Anti-Neutrophil Cytoplasmic Antibodies): For vasculitis
Complement Levels (C3, C4): Low in certain immune-mediated nephropathies
Serum Protein Electrophoresis (SPEP): To screen for multiple myeloma
Genetic Testing: For inherited conditions like Alport syndrome or PKD
Hepatitis B and C Serology: Viral hepatitis can cause membranous nephropathy
Who Should Be Screened for CKD?
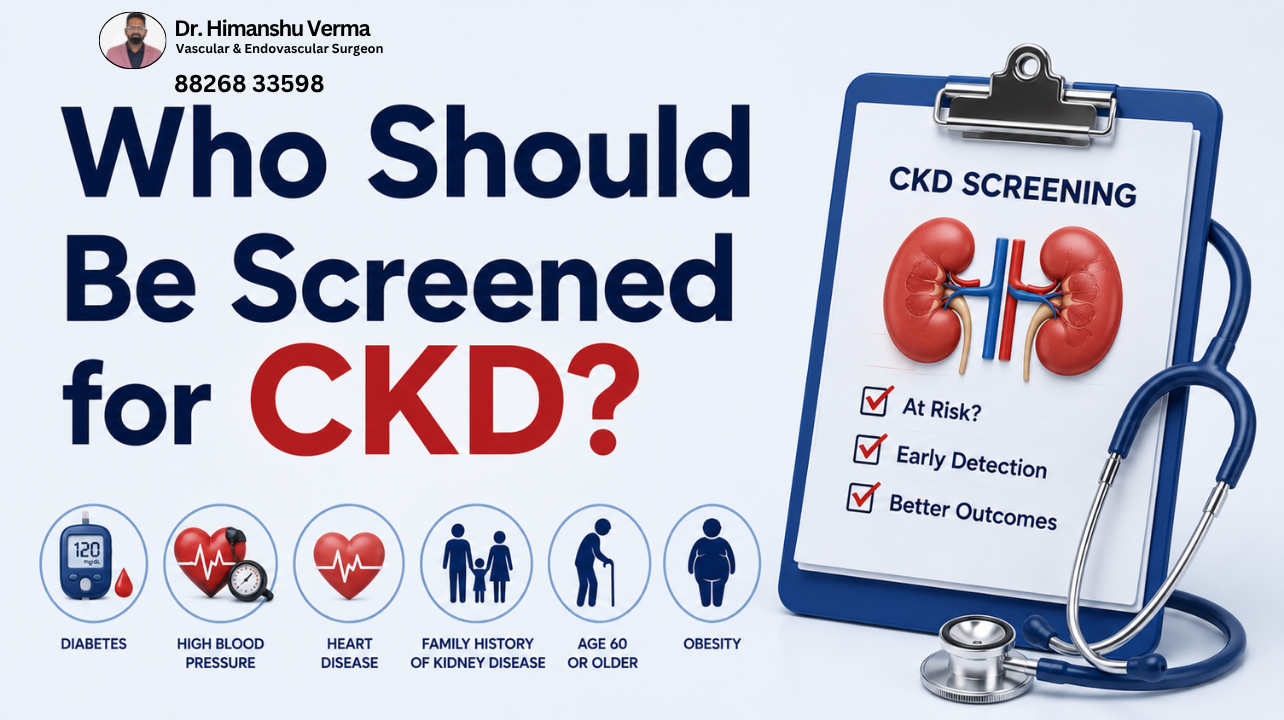
Chronic kidney disease screening for people with diabetes, high blood pressure, heart disease, obesity, or family history.
Blood tests for chronic kidney disease including CBC, serum creatinine, electrolytes, and eGFR.
The following individuals are at significantly elevated risk and should undergo periodic screening even without symptoms:
Individuals with Type 1 or Type 2 Diabetes (annual screening from the time of diagnosis)
Those with high blood pressure (hypertension), especially if poorly controlled
People with a family history of kidney disease or inherited kidney conditions
Individuals above 60 years of age
Those who have experienced a previous episode of acute kidney injury
People with cardiovascular disease (heart attack, stroke, peripheral arterial disease)
Individuals with obesity or metabolic syndrome
Those with a history of recurrent urinary tract infections or kidney stones
Long-term users of NSAIDs or nephrotoxic medications
Patients with structural urological abnormalities
Screening in these groups involves a simple urine test (for protein) and a blood test (for creatinine/eGFR) — both of which can be done at any pathology laboratory without a hospital visit.
How Dr. Himanshu Verma Supports CKD Patients
While the primary management of CKD falls under the expertise of nephrologists, a significant subset of CKD cases has an underlying vascular cause — or is significantly complicated by vascular disease. This is where Dr. Himanshu Verma's expertise becomes relevant.
As a skilled vascular surgeon practising in Gurgaon, Dr. Verma specialises in evaluating and treating conditions that affect blood supply to the kidneys and the cardiovascular complications that accompany advanced CKD:
Renal Artery Stenosis: A correctable vascular cause of CKD that often goes undiagnosed. Dr. Verma can evaluate renal blood flow using Doppler ultrasound and angiography, and recommend appropriate intervention — angioplasty, stenting, or surgical revascularisation — to restore adequate renal perfusion.
Access Creation for Dialysis: Patients progressing towards Stage 5 CKD require either an arteriovenous (AV) fistula or an AV graft for haemodialysis access. Timely creation of a well-functioning vascular access is critical to ensure smooth dialysis initiation. Dr. Verma performs these procedures with precision and care.
Cardiovascular Risk Management: CKD dramatically increases the risk of cardiovascular events — heart attacks and strokes are the leading causes of death in CKD patients. Peripheral arterial disease (PAD), which Dr. Verma manages extensively, is both a companion condition and a complication of CKD.
Peritoneal Dialysis Catheter Placement: For patients who choose peritoneal dialysis over haemodialysis, surgical placement of a peritoneal catheter is required — another procedure within Dr. Verma's expertise.
Dr. Verma works collaboratively with nephrologists to ensure that CKD patients receive holistic, multidisciplinary care addressing both renal function and vascular health.
Frequently Asked Questions About CKD Diagnosis
Q: Can CKD be diagnosed with just a single blood test? No. A single elevated creatinine or reduced eGFR reading is not sufficient. The result must be confirmed on at least two separate occasions, at least three months apart, to establish chronicity. A urine test for protein is equally important.
Q: My urine creatinine is high. Does that mean I have CKD? Urine creatinine is not the same as serum (blood) creatinine and does not directly indicate kidney disease. What matters is the serum creatinine used to calculate eGFR, and the urine albumin-to-creatinine ratio (UACR). Please consult a doctor for proper interpretation.
Q: Is CKD the same as kidney failure? No. CKD encompasses a spectrum of five stages. Only Stage 5 — end-stage renal disease — constitutes kidney failure requiring dialysis or transplantation. Many patients with CKD in earlier stages live long, healthy lives with appropriate management.
Q: Can CKD be reversed? In most cases, CKD involves irreversible damage. However, its progression can be significantly slowed — or in some cases halted — with proper treatment of the underlying cause, blood pressure control, glucose management, and lifestyle changes.
Q: How often should CKD patients be tested? Frequency depends on the stage of CKD. In general, patients with Stage 3 CKD should have eGFR and UACR checked at least once every six months. Higher-stage patients require more frequent monitoring.
A Final Word: Don't Wait for Symptoms
Chronic kidney disease is a condition that robs people of time — because by the time noticeable symptoms appear, significant and irreversible damage may already have occurred. Foamy urine, a high creatinine on a routine blood test, or blood pressure that is suddenly difficult to control should never be ignored.
Timely diagnosis of CKD — through the combination of urine analysis, blood tests, and imaging — gives patients the best possible opportunity to protect their remaining kidney function, prevent complications, and maintain quality of life.
If you or someone in your family falls into a high-risk group, or if your recent reports have shown elevated creatinine or protein in the urine, it is time to act.
For consultations and further evaluation, you can reach Dr. Himanshu Verma's clinic in Gurgaon. Early assessment, the right diagnostic workup, and a personalised care plan can make all the difference.